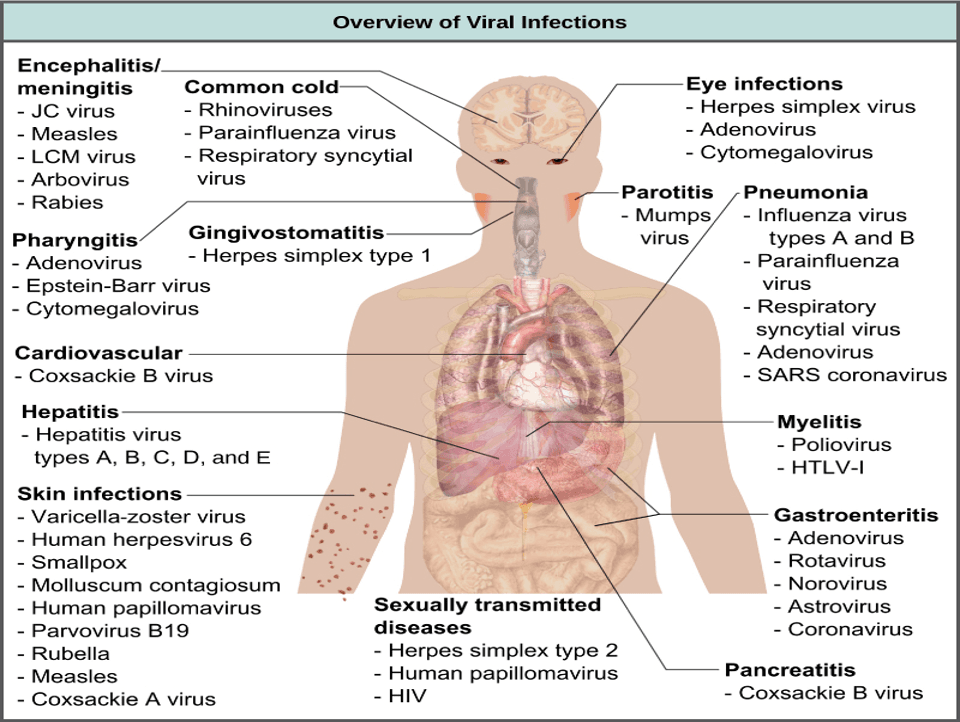
Transmission of human viral diseases
The transmission of human viral diseases occurs through various routes, depending on the virus’s characteristics and the host’s interaction with the environment.
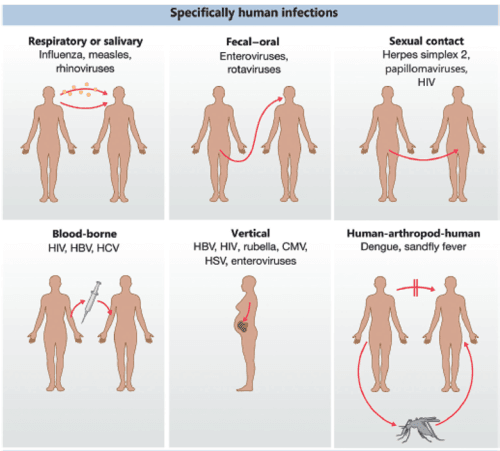
1. Direct Contact
- Physical Contact: Includes skin-to-skin contact, kissing, or sexual activity.
- Examples: Herpes simplex virus (HSV), Human papillomavirus (HPV).
- Vertical Transmission: From mother to child during pregnancy, childbirth, or breastfeeding.
- Examples: HIV, Hepatitis B virus (HBV), Zika virus.
2. Respiratory (Droplet or Airborne)
- Droplet Transmission: Large respiratory droplets from coughing, sneezing, or talking, which travel short distances.
- Examples: Influenza, SARS-CoV-2.
- Airborne Transmission: Aerosolized particles that remain suspended in the air for long periods and travel farther distances.
- Examples: Measles virus, Varicella-zoster virus.
3. Fecal-Oral Route
- Spread through ingestion of contaminated food, water, or contact with fecal matter.
- Examples: Rotavirus, Hepatitis A virus, Norovirus, Poliovirus.
4. Vector-Borne Transmission
- Arthropods: Transmitted via bites from infected mosquitoes, ticks, or other vectors.
- Examples: Dengue virus, West Nile virus, Yellow fever virus, Chikungunya virus.
5. Bloodborne Transmission
- Through contact with infected blood or body fluids via transfusion, sharing needles, or medical procedures.
- Examples: HIV, HBV, Hepatitis C virus (HCV).
6. Zoonotic Transmission
- Spread from animals to humans through direct contact, consumption of contaminated animal products, or intermediate hosts.
- Examples: Rabies virus, Hantavirus, Ebola virus, Coronaviruses (e.g., SARS-CoV, MERS-CoV).
7. Iatrogenic Transmission
- Caused by medical procedures, such as organ transplantation, contaminated instruments, or improperly sterilized equipment.
- Examples: Creutzfeldt-Jakob disease (prion-related), HBV, HCV.
8. Environmental (Fomites and Surface Contact)
- Indirect transmission through contaminated surfaces or objects.
- Examples: Rhinovirus (common cold), Norovirus.
Factors Influencing Transmission
- Viral load and shedding patterns.
- Host immunity and susceptibility.
- Environmental conditions (temperature, humidity).
- Preventive measures (vaccination, hygiene).
Each route highlights the importance of targeted public health measures like vaccination, sanitation, vector control, and education to mitigate disease spread.
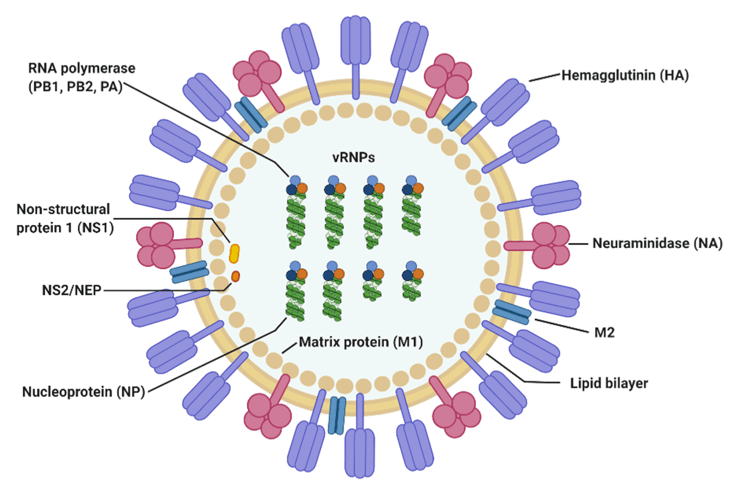
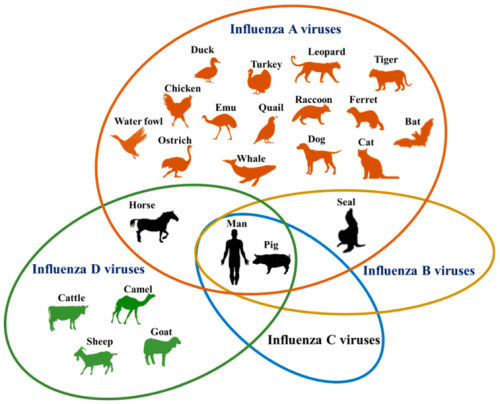
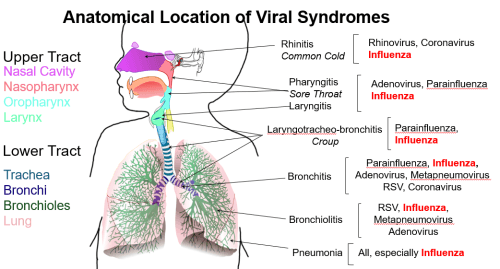
1. Influenza (A, B, C and D)
- Causative Agent: Influenza virus
- Group V: Negative sense ssRNA viruses
- Family: Orthomyxoviridae
- Genera
- Alphainfluenzavirus: Influenza A virus (is most significant in pandemics)
- Betainfluenzavirus: Influenza B virus
- Gammainfluenzavirus: Influenza C virus
- Quaranjavirus: Quaranfil quaranjavirus
- Thogotovirus
- Transmission
- Respiratory droplets (primary route).
- Contact with contaminated surfaces or fomites.
- Interspecies transmission of influenza A viruses
- Replication Cycle
- Virus binds to host cell receptors (sialic acid residues).
- Endocytosis and uncoating.
- RNA replication in the nucleus.
- Assembly and release by budding.
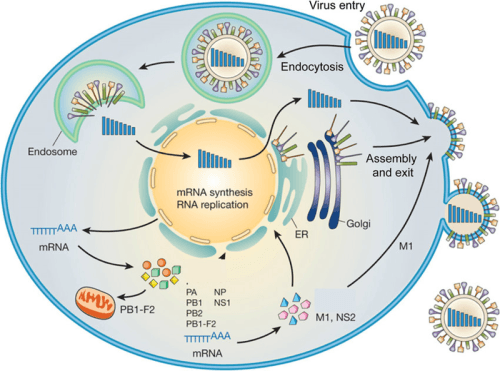
- Pathogenesis
- Neuraminidase (NA) degrades protective mucus
- Hemagglutinin (HA) binds cell surface receptors
- Viral replication kills host cells
- Infects respiratory epithelial cells, leading to necrosis, inflammation, and cytokine release.
- Clinical Signs
- Fever, cough, sore throat, fatigue, muscle aches, and nasal congestion.
- Control
- Annual vaccination (inactivated or live-attenuated).
- Antiviral drugs (e.g., oseltamivir, zanamivir).
- Good hygiene and respiratory etiquette.
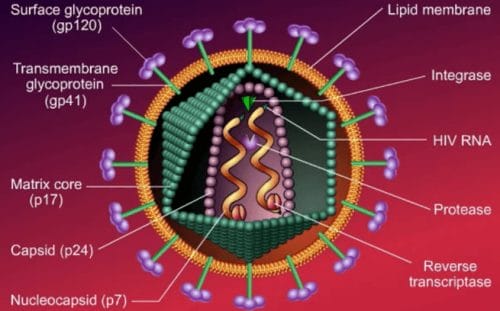
2. Human Immunodeficiency Virus (HIV)
- Causative Agent: Human immunodeficiency virus 1 and 2 (HIV-1 and HIV-2)
- Group VI: Positive sense ssRNA with DNA intermediate viruses
- Family: Retroviridae
- Genus: Lentivirus
- Transmission
- Sexual contact, blood, needle sharing, mother-to-child (perinatal or breastfeeding).
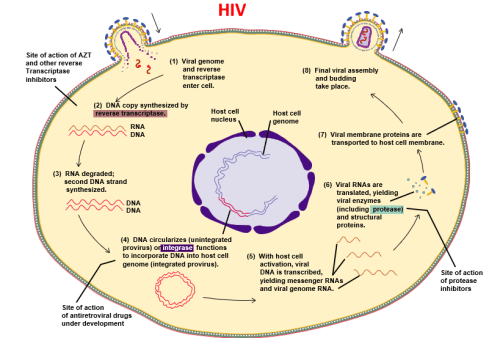
- Replication Cycle
- Virus binds CD4 and co-receptors (CCR5/CXCR4).
- Reverse transcription of RNA into DNA.
- Integration into the host genome.
- Assembly and release of virions.
- Pathogenesis
- Progressive depletion of CD4+ T cells due to destruction of cells in three ways, leading to immunodeficiency.
- Viral replication leaves holes in cell membranes
- Infected cells fuse with other cells
- Combine to form a syncytium that destroys all affected cell
- Antibodies against HIV bind to the infected cells and activate the complement system, which destroy the infected cells
Consequences
- All daughter cells from infected cell are infected
- Genetic codes can direct the cell to make HIV
HIV T Cell Count
- HIV destroys about 1 billion CD4+ T cells every day
- Normal T cell count: 800-1200 cells/ul
- T cell count >500; generally healthy
- T cell count 200-499; minor immune problems
- Immune problems start when CD4+T cell counts drop below 500 cells/μl
- T cell count <200; severe problems
HIV genetic variability
- HIV differs from many viruses in that it has very high genetic variability
- This is due to its fast replication cycle, with the generation of about 1010 virions every day
- This is coupled with a high mutation rate of approximately 3 x 10−5 per nucleotide base per cycle of replication
- Mutation is also caused by recombinogenic properties of reverse transcriptase
- This complex scenario leads to the generation of many variants of HIV in a single infected patient in the course of one day
- This variability is compounded when a single cell is simultaneously infected by two or more different strains of HIV
- Clinical Signs
- Early: Flu-like symptoms (acute retroviral syndrome).
- Late: Opportunistic infections, cancers, and AIDS.
- Control
- Antiretroviral therapy (ART) to suppress viral replication.
- Safe sex practices and harm reduction strategies.
- Prevention of mother-to-child transmission (PMTCT).
3. Hepatitis Viruses
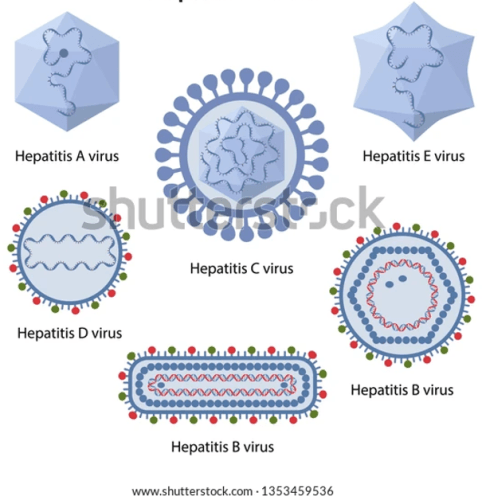
Hepatitis A
- Causative Agent: Hepatitis A virus (HAV)
- Family: Picornaviridae
- Genus: Hepatovirus
- Transmission: Fecal-oral route (contaminated water/food).
- Clinical Signs: Jaundice, abdominal pain, nausea.
- Control: Vaccination, improved sanitation.
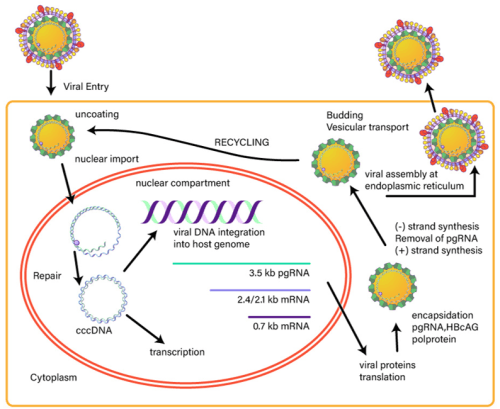
Hepatitis B
- Causative Agent: Hepatitis B virus (HBV)
- Family: Hepadnaviridae
- Genus: Orthohepadnavirus
- Transmission:
- Blood, sexual contact, mother-to-child, contaminated needles.
- Replication Cycle
- Entry via NTCP receptor on hepatocytes.
- Reverse transcription in the cytoplasm.
- Formation of covalently closed circular DNA (cccDNA).
- Assembly and release of virus.
- Pathogenesis
- Chronic infection causes immune-mediated liver inflammation and fibrosis, progressing to cirrhosis or hepatocellular carcinoma (HCC).
- Clinical Signs
- Acute: Jaundice, dark urine, abdominal pain, fatigue.
- Chronic: Often asymptomatic until liver complications arise.
- Control
- HBV vaccine (recombinant).
- Antiviral therapy for chronic cases (e.g., entecavir, tenofovir).
- Safe blood handling and hygiene.
Hepatitis C
- Causative Agent: Hepatitis C virus (HCV)
- Family: Flaviviridae
- Genus: Hepacivirus
- Transmission: Bloodborne (needles, transfusion).
- Control: Antiviral therapy (direct-acting antivirals).
| TYPES | HEPATITIS A | HEPATITIS B | HEPATITIS C | HEPATITIS D | HEPATITIS E |
| Mode of transmission | Fecal route | Contact(blood) | Contact(blood) | Contact(blood) | Fecal route |
| Classification | Picornaviridae | Hepadnaviriae | Flaviviridae | Deltaviridae | Caliciviridae |
| Incubation | 2-6 Weeks | 2-6 Months | 2 weeks – 6 Months | 60 – 180 days | 21-24 days |
| Chronic infection | NO | YES | YES | YES | NO |
| Clinical outcome of chronic infection | NO | Cirrhosis or hepatocellular carcinoma | Cirrhosis or hepatocellular carcinoma | Co infection | NO |
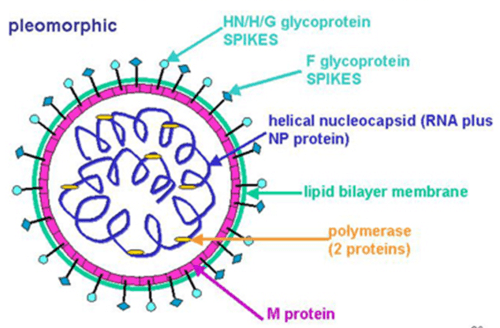
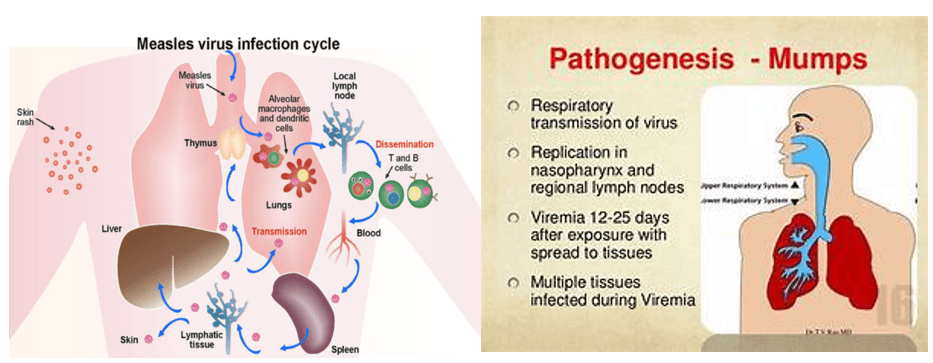
4. Measles and Mumps
- Causative Agent: Measles virus (Measles) and Mumps virus (Mumps)
- Group V: Negative sense ssRNA viruses
- Family: Paramyxoviridae
- Genus: Morbillivirus
- Morbilivirus – Measles morbillivirus (measles virus)
- Respirovirus – Human parainfluenza virus 1 and 3
- Rubulavirus – Human parainfluenza virus 2 and 4 -Mumps virus
- Transmission
- Measles virus is a highly contagious virus that lives in the nose and throat mucus of an infected person. It can spread to others through coughing and sneezing (Airborne droplets). Measles virus can live for up to two hours in an airspace after an infected person leaves an area
- Mumps is a contagious disease that is caused by mumps virus. Most people will have swelling of their salivary glands
- Replication Cycle
- Binds to SLAM/CD46 receptors on immune cells.
- Cytoplasmic replication via RNA-dependent RNA polymerase.
- Budding or cell-cell spread.
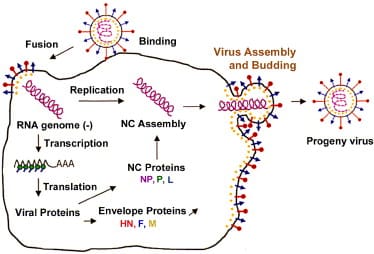
- Pathogenesis
- Replication in respiratory epithelium, viremia, and immune suppression.
- Receptor: CD46 on surface of macrophages
- Rash-cytotoxic T cells attacking the virus infected vascular endothelial cells in the skin
- CMI- neutralizing the virus during viremic phase
- MOT: droplet inhalation
- Hematogenous transplacental
- Clinical Signs
- Fever, cough, coryza, conjunctivitis (3 C’s), Koplik spots, maculopapular rash.

- Control
- Prevent measles and mumps with MMR vaccine (measles, mumps, and rubella)
- Isolation during outbreaks.
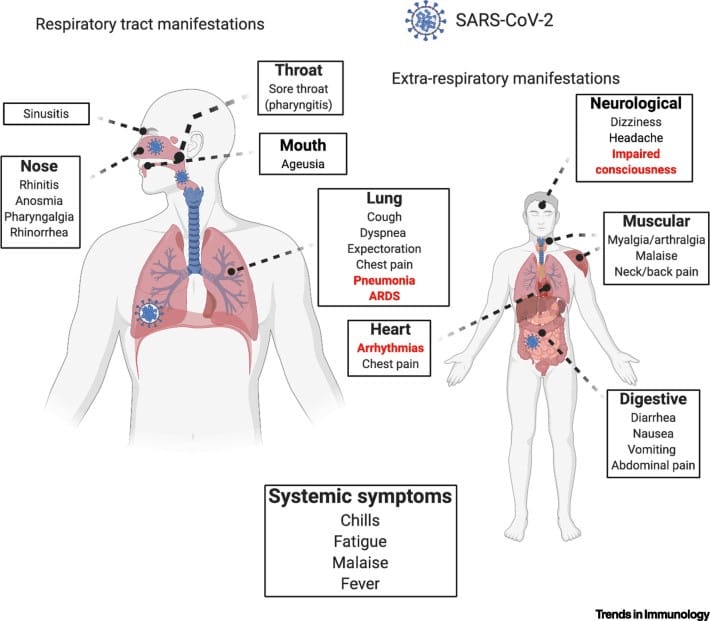
5. COVID-19
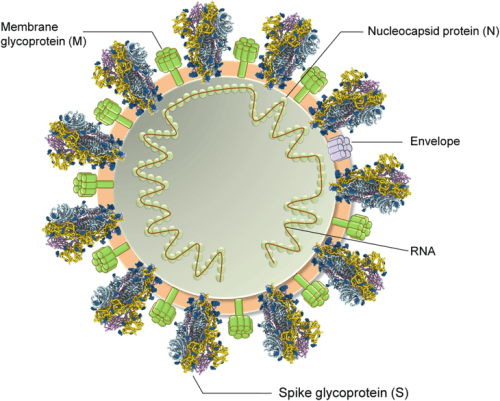
- Causative Agent: Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2)
- Group IV: Positive sense ssRNA viruses
- Family: Coronaviridae
- Genus: Betacoronavirus
- Other viruses: Middle East respiratory syndrome coronavirus (MERS-CoV); Severe Acute Respiratory Syndrome coronavirus 1 (SARS-CoV-1)
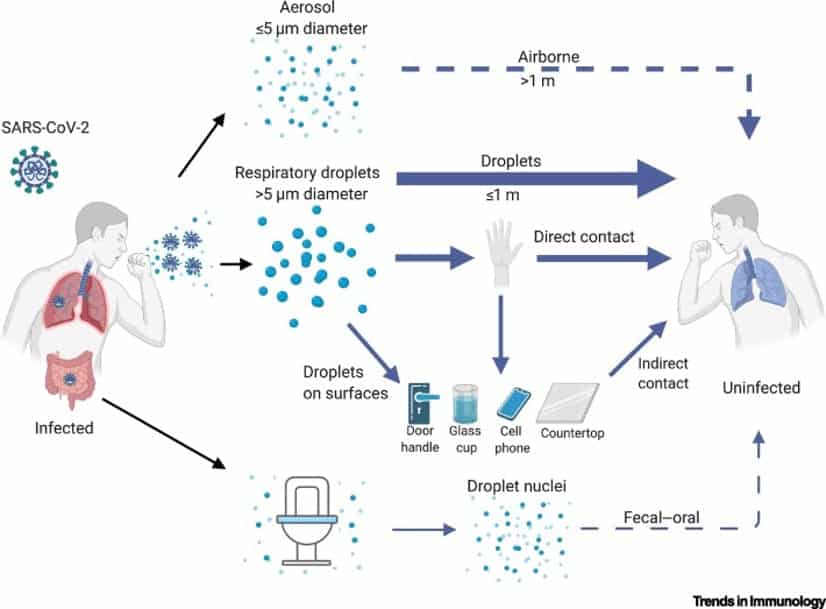
- Transmission
- Respiratory droplets, aerosols, fomites.
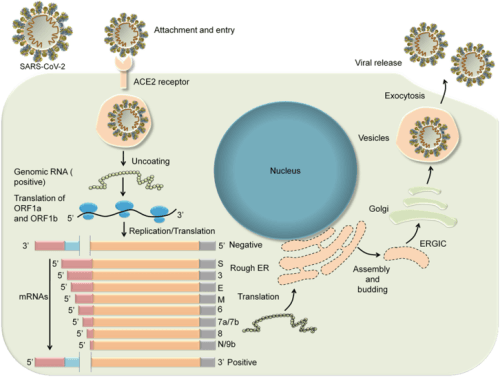
- Replication Cycle
- Binding to ACE2 receptors.
- RNA replication in cytoplasm.
- Assembly in the ER-Golgi complex.
- Release via exocytosis.
- Pathogenesis
- Respiratory epithelial damage, hyperinflammation, and cytokine storm in severe cases.
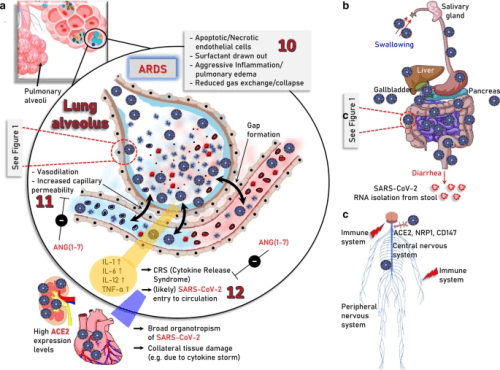
- Clinical Signs
- Fever, cough, loss of smell/taste, shortness of breath, severe ARDS in critical cases.
- Control
- Vaccination (mRNA and viral vector vaccines).
- Masking, social distancing, and hygiene.
- Antivirals (e.g., remdesivir) and monoclonal antibodies.
6. Dengue Fever
- Causative Agent: Dengue virus (DENV 1–4)
- Family: Flaviviridae
- Genus: Flavivirus
- Transmission: Aedes aegypti mosquitoes.
- Replication Cycle: Virus enters via receptor-mediated endocytosis → cytoplasmic replication → assembly in ER → release.
- Pathogenesis: Capillary leakage, hemorrhage, immune-mediated enhancement (severe cases).
- Clinical Signs: Fever, rash, severe headache, joint/muscle pain, hemorrhagic shock (severe cases).
- Control: Mosquito control, supportive care, vaccine (Dengvaxia for endemic areas).
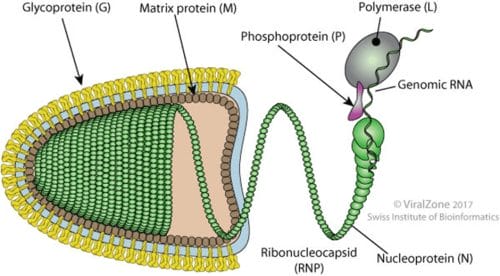
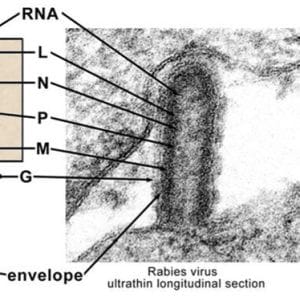
7. Rabies
- Causative Agent: Rabies virus
- Group V: Negative sense ssRNA viruses
- Family: Rhabdoviridae
- Genus: Lyssavirus
- Transmission: Saliva of infected animals via bites.
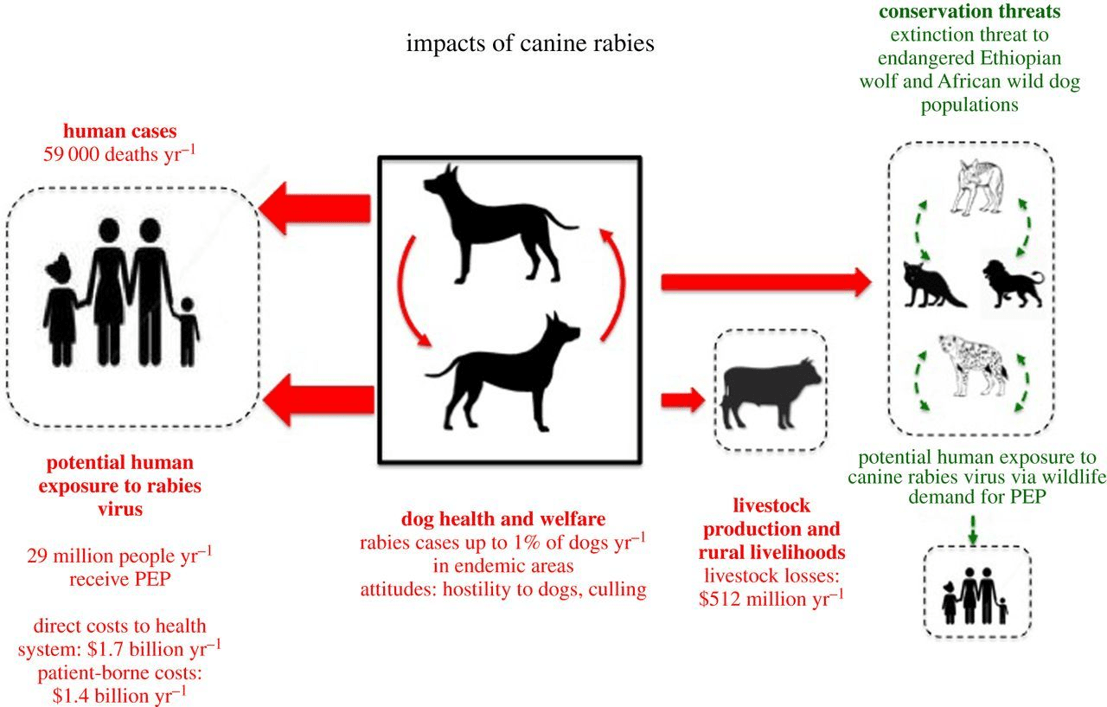
- Replication
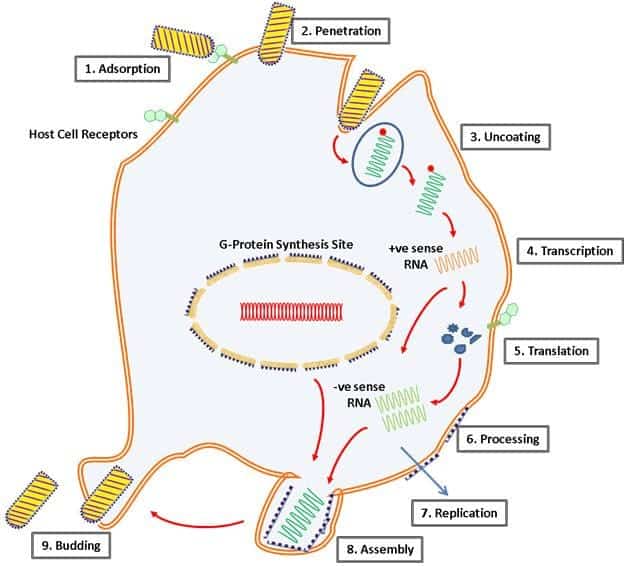
- Pathogenesis: Virus travels via peripheral nerves to CNS → encephalitis.
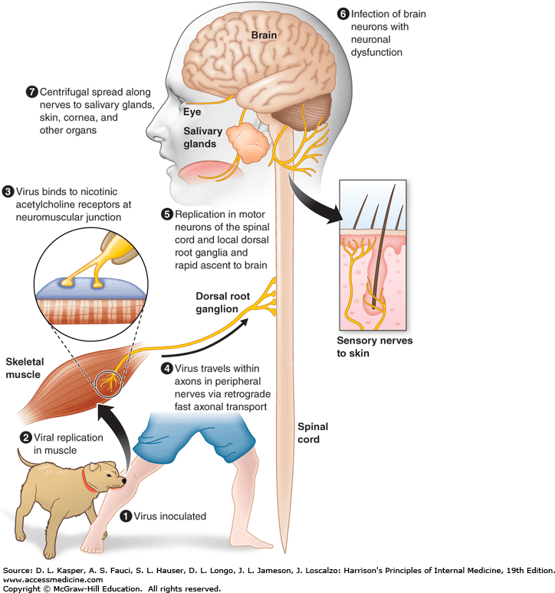
- Clinical Signs: Hydrophobia, agitation, paralysis, coma, death.
- Control: Post-exposure prophylaxis (PEP), vaccination of pets.
8. Polio
- Causative Agent: Poliovirus
- Group V: Positive sense ssRNA viruses
- Family: Picornaviridae
- Genus: Enterovirus
- Transmission: Poliovirus is very contagious and spreads through person-to-person by contact. Fecal-oral route. It lives in an infected person’s throat and intestines.
- Pathogenesis: Replicates in gut, spreads to CNS causing motor neuron destruction.
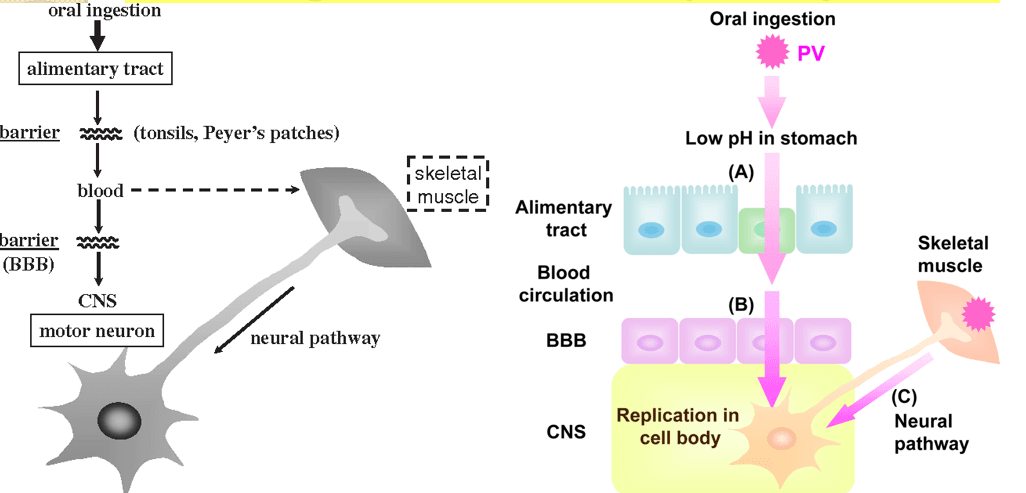
- Clinical Signs: Asymptomatic, febrile illness, or paralysis.
- Meningitis – infection of the spinal cord and or brain)
- Paralysis (can’t move parts of the body) or weakness in the arms, legs, or both. Paralysis is the most severe symptom can lead to permanent disability and death. Polio has been around since ancient times.

- Control: Vaccination (IPV, OPV).
9. Human Herpesviruses
- Group I: dsDNA viruses
- Family: Herpesviridae
- Subfamily: Alphaherpesvirinae
- Herpes simplex virus type 1 and 2 (HSV-1 and HSV-2)
- Varicella-zoster virus VZV
- Subfamily: Betaherpesvirinae
- Cytomegalovirus CMV
- Human herpesvirus type 6 HHV-6
- Human herpesvirus type 7 HHV-7
- Subfamily: Gammaherpesvirinae
- Epstein-Barr virus EBV
Herpes Simplex Virus (HSV-1, HSV-2)
- Family: Herpesviridae
- Genus: Alphaherpesvirus
- Transmission: Direct contact with lesions, saliva, or genital secretions, skin and oropharyngeal lesions and carriers.
- Clinical Signs: HSV-1 infect the upper part of the body (mouth and the face) leading to cold sores. HSV-2 infect the lower part of the body (genital infections) leading to genital ulcers. There is little cross protection and therefore, you can get both infections.
- Control: Antiviral drugs (acyclovir).
Varicella-Zoster Virus (VZV)
- Disease: Chickenpox, shingles.
- Transmission: Respiratory droplets or direct contact with lesions.
- Pathogenesis of HSV 1 and 2
- Varicella (Chicken pox) primary infection usually in childhood.
- Zoster (shingle) -Reactivation of early varicella)
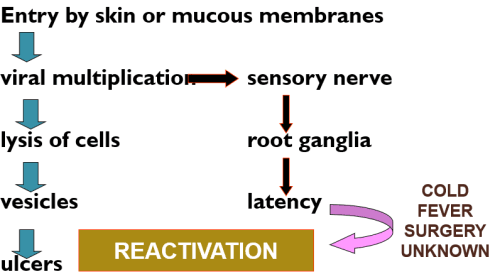
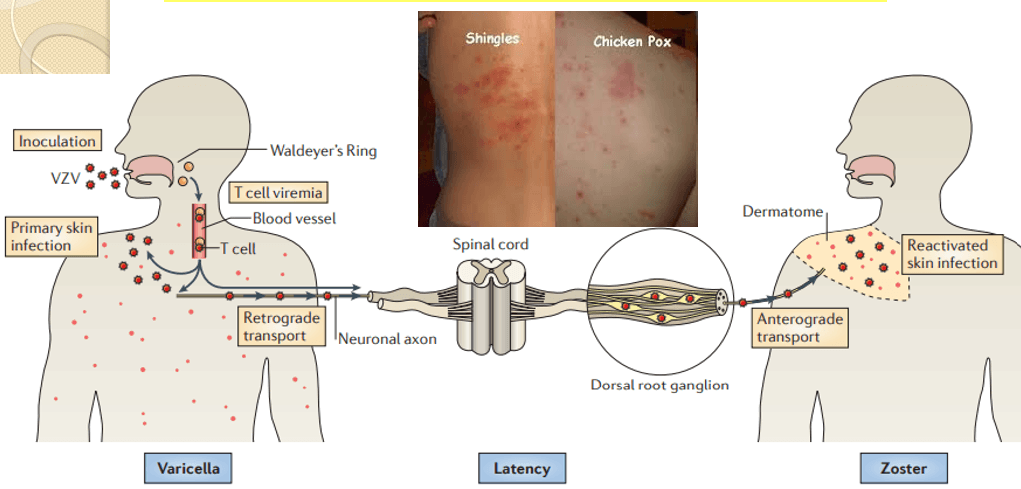
- Control: Vaccination (varicella, zoster vaccines).
Human Papilloma
- Causative agent: Human Papilloma Viruses
- Group I: dsDNA viruses
- Family: Papillomaviridae
- Genera:
- Alphapapillomavirus
- Betapapillomavirus
- Gammapapillomavirus
- Mupapillomavirus
- Nupapillomavirus
All these genera are for human but there are many genera for other animals as well
- Transmission:
- Sexual contact: Most common route, including vaginal, anal, and oral sex.
- Non-sexual contact: Direct contact with infected skin or mucosa.
- Vertical transmission: From mother to child during childbirth, potentially causing respiratory papillomatosis in infants.
- Pathogenesis: Infection of basal epithelial cells: HPV gains entry through microabrasions in the skin or mucosa.
- The pathogenesis of HPV infection in thoracic visceral lungs
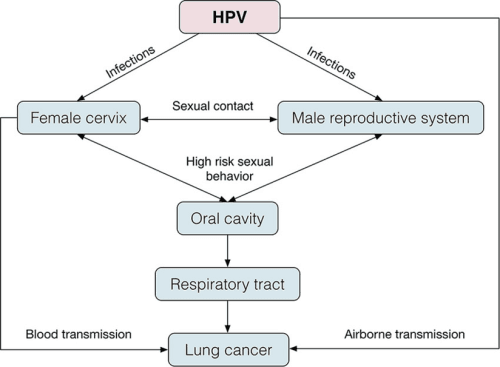
- Pathogenesis of HPV in cervical cancer
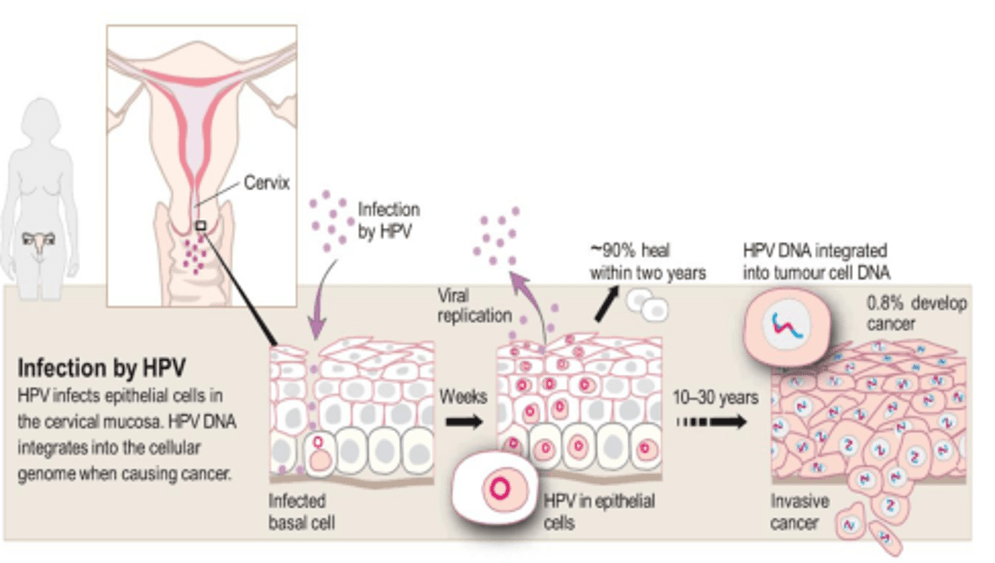
- Replication: Virus integrates into host cells and uses host machinery to replicate.
- Oncogenesis (High-risk types):
- HPV E6 protein: Inhibits tumor suppressor p53, leading to reduced apoptosis.
- HPV E7 protein: Inactivates tumor suppressor Rb, promoting uncontrolled cell proliferation.
- This process increases the risk of progression to cancer.
- Clinical Manifestations
- Warts (Low-risk types):
- Common warts (hands and feet).
- Anogenital warts (condylomata acuminata).
- Precancerous lesions and cancers (High-risk types):
- Cervical intraepithelial neoplasia (CIN).
- Cervical cancer, oropharyngeal cancer, anal cancer, and penile cancer.
- Warts (Low-risk types):
- Prevention
- Vaccination: Highly effective vaccines available (e.g., Gardasil, Cervarix). Protects against high-risk types (e.g., 16, 18) and low-risk types (e.g., 6, 11). Recommended for both males and females, ideally before the onset of sexual activity.
- Safe sexual practices: Use of condoms can reduce, but not eliminate, risk.
- Regular screening: Pap smears and HPV testing are critical in preventing cervical cancer.
- Treatment
- For warts: Topical treatments: Salicylic acid, imiquimod. Cryotherapy or surgical removal.
- For precancerous lesions and cancers: Surgical excision, radiotherapy, or chemotherapy depending on the stage.
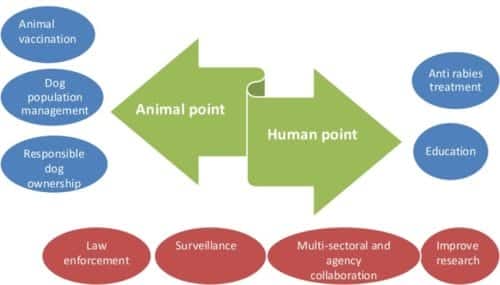
General Strategies for Viral Disease Control
- Vaccination
- Most effective preventive tool (e.g., measles, polio, influenza, HPV).
- Antiviral Drugs
- Target specific viral replication steps (e.g., ART for HIV, oseltamivir for influenza).
- Hygiene and Sanitation
- Handwashing, proper waste disposal.
- Vector Control
- Mosquito control for arboviruses (e.g., dengue, Zika).
- Public Health Measures
- Surveillance, isolation, and quarantine during outbreaks.
- Education
- Promote awareness and preventive measures.